
I’m using ADE to mean any effect whereby those who took a “vaccine” end up being more susceptible to the virus. That is a problem for those who took the genetic therapy (falsely called vaccine) for covid, because in animal studies developing a coronavirus vaccine, it appears that most or all of the animals died within 2 years from ADE. And, to make it all much worse, not only doesn’t anyone have a very clear idea about the mechanism, but they skipped the necessary trials for the covid therapy to see if it would happen and they appear to have no idea how to treat it, if it does occur.
I would suggest, the risk of covid ADE developing due to the therapies, is akin to walking across a busy road with a blind fold and ear muffs on. If you were over 80 with multiple relevant health issues then, yes, perhaps it might have been the right choice to take the … I almost called it “death therapy” … because to be blunt, the life expectancy of an over 80 with health issues it already bad, and even a very bad decision about a covid therapy does not massively change that prognosis. But if you are under 50, and especially any child, then it is just insanity!! And even if ADE does not develop, we MUST prosecute those who took the insane decision, not just to allow children, but to FORCE them to take this appalling therapy.
Present position
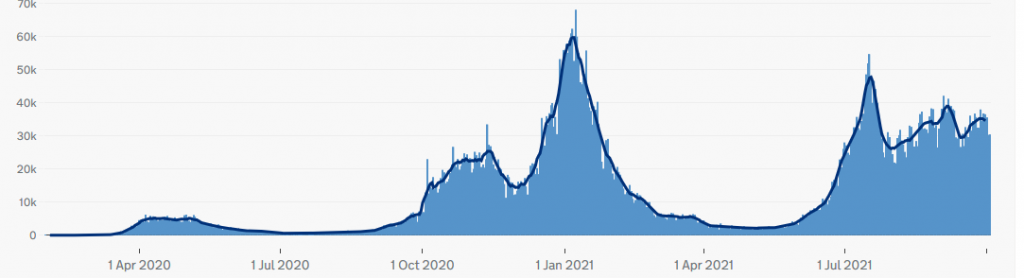
Above is the latest graph of positive tests in the UK. The important thing is that it can be clearly seen that there was a spring 2020 epidemic where tests clearly rose and then clearly fell as immunity to that variant reached the level for community immunity, an Autumn 2020 epidemic, then a spring 2021 epidemic. In each of these cases, the number of people testing positive virus grew exponentially and then declined exponentially. This fits a model of community immunity, which is the level of immunity which causes a virus to tend toward zero in a real community, where interactions are not random. This is a lower level than “herd immunity”, which is a theoretical model of wild animals with no social memory and so randomised interactions. Or as I put it, a man in such a society has as much chance as sleeping with his wife as with the PM.
Once community immunity is reached, three things can trigger a new epidemic:
- A new variant (where present immunity has less protection)
- A change in the way people interact (so that the virus can move about via new pathways which are not blocked by an individual who already has immunity).
- Reducing immunity
Which, brings me on to the present. As can be seen, the UK in general saw a typical rise of positive tests in July. This was almost certainly due to the arrival of the Indian variant, which bypassed previous immunity … but also has a much lower death rate. However, the very worry aspect is that whereas every previous epidemic rose to a peak, then dropped away exponentially, the latest peak did no such thing. Instead, we now see a continual background level of positive tests which clearly shows a change in behaviour.
Explaining the change in behaviour
Looking at the available statistics, it appears that this ongoing trend is created by a number of smaller, more localised epidemics which have occurred in Scotland and now Wales as well as the north of England. The first thing I have to say here is that Scotland and Wales are still being mad about covid. And, to my eyes, it appears that this insanity is only INCREASING the spread**.
However, the important thing is the change in behaviour away from nation wide epidemics, to smaller regional ones. To my eyes, this looks like the pattern of outbreak we get in wild fires … where fire tends to burn the areas which have not recently had fire, but they miss areas that have recently had fires. So, this is what occurs, when something is steadily increasing the susceptibility generally (brush growing), but the pattern is affected by previous epidemics (so a repeat of the same Indian variant).
So, it appears that immunity and/or susceptibility is increasing. This could be because of:
- The covid therapy does not provide long term protection (great for repeat sales)
- That people naturally change their behaviour over time … which opens up new pathways for the virus, until there are sufficient to create an epidemic (so a lockup after a peak, actually INCREASES the chance of infection by reconfiguring the way people socialise AFTER the present pathways were blocked).
- Related to (2) that we are moving into Autumn, when people change their behaviour, not only reconfiguring social relationships, but also the virus is easier to spread.
- That a new variant has emerged (for which there is no evidence)
- That ADE is developing.
ADE?
It is now approaching a year since the very first people got their covid therapy. Whatever interpretation we have for the series of mini outbreaks, falling immunity seems to be occurring, so we would not expect to start seeing signs of ADE until now. And, the lab animals died when immunity dropped and within 2 years. So, the critical period would appear to be this and next winter. If ADE does not develop by spring of 2023 … society has managed to walk across the busy road and peak hour blind folded with ear muffs and will appear to have got to the other side without mass die off.
However, the first condition to suggest ADE is developing … which is repeated smaller outbreaks indicating lowering immunity has occurred.
The next condition is that the rate of infection amongst those who took the jab falls at a rate either reaching or suggesting it will reach a stage whereby those who took the jab are more likely to be infected than those who did not. There is some evidence from a small sample of Scottish deaths, that this has already occurred.
The next condition, is that the higher rate of infection/death in those who took the covid therapy, cannot be explained in other ways … in particular, those who took the jab first were the vulnerable who were most likely to die in the next year. Because there was a delay of many months between the first vulnerable groups, and those far less likely to die, a high death rate amongst those who got the covid therapy, cannot be translated into “ADE is developing” unless we start seeing large numbers of healthy middle aged people dying … and only those who took the jab and that may take another six months. Unfortunately, we just aren’t being given the data to tell us if this is happening (which is in itself highly indicative that it may be happening … because if it weren’t happening, they would be happy to publish the data!)
This leaves the final condition: that the susceptibility to repeat infections from covid continues to increase. Unfortunately, coming into winter, we already expect an increase in infections, so how can we tell the difference? The only real difference, is that if ADE is not occurring, then we will see another drop in the level of infections down to zero, but if ADE is making people more and more susceptible, we will continue to see a background level of covid infections … with repeated local epidemics … but whilst sometimes lulling, in general I expect an overall increasing level of severity … over the next year. But, that could be confused with a new variant … so … to put it simply, I went to visit my own family and make peace given the real possibility, that we could be in a new lockup soon which could develop into the worse tragedy in humanity.
On, the other hand … it might not … but like the comet that passes the planet of the caveman and nearly wipes out humanity … they’ll never know how close they came … and they wouldn’t believe me even if I told them.
What if ADE occurs?
The animal studes were for more deadly strains of coronavirus. This might be good news, as it might mean that the coronavirus needs to be a lot more deadly than the covid-flu, to cause mass die off. On the other hand, if ADE effectively turns off the immune system, then even very benign variants could become deadly, which might mean that covid is just as deadly as the animal studies.
The next thing, is that I’ve heard nothing about anyone trying to treat animals that developed ADE. So, it is possible that there are very simple treatments that reverse the process. But it is also possible that there is none.
Covid was almost exclusively a killer of the old with multiple conditions. As such we might expect ADE to be most deadly to the old with multiple conditions. However, bizarrely, it could be the reverse: that the old with failing immune systems, don’t get the effect, whereas the young do.
Hence my analogy of walking across a busy (and fast) road. We either get off Scot free (and largely ignorant of the huge risk taken), or we could get walloped by a broadside with no chance of most people surviving. Or … anything in between. ADE might just appear as a slightly higher death rate, which no one notices until they do proper research after the present brain dead people who led us into this terrible situation are long gone.
**I suspect what is happening is that masks are catching large droplets of mucous that would fall rapidly onto a surface, and instead the droplets are drying on the masks and then the movement is causing the dried mucous to break apart into an incredibly fine dust which is ideally suited to going straight through the pathetic masks which people wear day in day out.
