
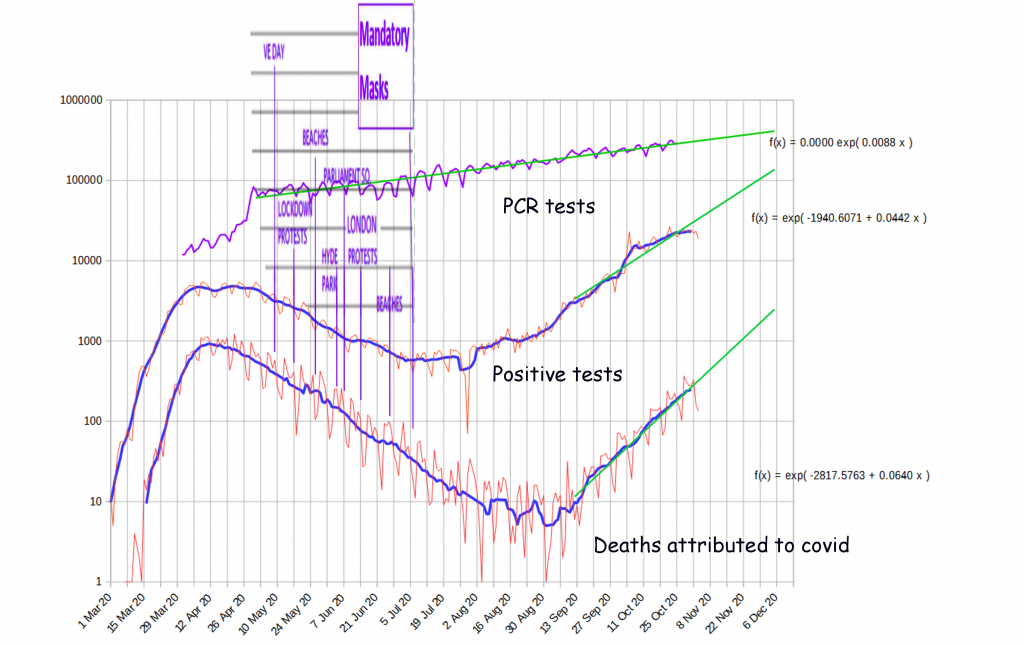
This post is trying to explain the main features of the epidemic as shown in the following curve (and the contrast between deaths in countries with lockup and not)
- As the log vs. time curve shows, the epidemic either is increasing or decreasing in straight lines, meaning exponential increase/decrease and these DO NOT RESPOND AT ALL to policy changes
- That the only other significant feature that can respond to policy is the turning point
- That countries that locked up like the UK, Spain, Peru have a MUCH HIGHER death rate than countries who do not lockup.
- That there was an (apparent) second wave
Bizarrely the problem here is not the lack of effect of policy – because it’s very easy to explain why masks didn’t work, or why anti-social policies like distancing had no effect (people ignored them), the problem is explain, BOTH how policy had no effect on the rate of spread of the virus, but also massively increased deaths.
I set out in “Lockups kill” a plausible explanation of why lockups tend to increase deaths in that they increase the fraction of social contact which is with vulnerable people who are far far more likely to die. But that requires that policy has an effect on how the virus spreads, whereas, the straight lines, which do not change as policy changes, appear to show that policy has no effect.
This obviously needed some kind of explanation.
Possibilities
One of the possibilities for a constant increase or decrease irrespective of policy changes, is that policy is having no affect on the mechanism by which the virus spreads. So I tried to think of potential mechanism that might work that way. This means we get it by an action we continue to do irrespective of the policy. They fall into the following:
- Breathing … that the virus is largely spread “on the wind” from house to house.
- Drinking … that the water we drink is infected
- Eating … that the food we eat is infected
If we are breathing it in, then possibly the virus is now mixing almost as part of the atmosphere and is becoming as ubiquitous as oxygen. The problem with this idea, is that it can only survive under sunlight for a limited time, which makes it difficult to cross the sea. So any (UK) community on a western coast with wind predominantly coming inland, ought to be largely free of the virus, and I cannot see evidence to support that.
If we are drinking it in, then perhaps large amounts of the virus are landing on the lakes and pools that store drinking water. But many of these are not open to the air, and if it were spreading that way, then the epidemic ought to be very patchy.
If it were being caught predominantly via the food we eat, then the most likely produce is fresh uncooked produce, and the most likely source of that is from foreign countries. As such, all countries with the same suppliers ought to have had an epidemic matching the epidemic in the supplying countries, which makes the lower death rate in Sweden hard to explain.
Another possibility is an intermediary host. I considered, birds, dogs, cats, rats, mice and even bedbugs, biting flying insects and skin mites, and none fit.
Back to humans
Having ruled out as unlikely all other possible causes (I could think of), I was left with the idea that the consistent growth/decline and the change in death rate, had all to do with humans. My first idea, was that perhaps most of the virus spread in a way that was unaffected by the lockup, but that a tiny fraction of interactions were affected. The idea, was that most of the epidemic growth/decline was occurring outside the control of lockup, but that a tiny fraction of interactions were impacted by lockup, but a change in them was having a very small impact on growth (too small to see). The problem with that, is that if we assume 99 social interactions are not affected by lockup, so the virus spreads as normal, the 1 that is, that perhaps links to a new community, means that a further 99 people do not catch the virus. So even though that 1 interaction is a small percentage of interactions, it still has a massive impact on the growth rate. So this simple idea didn’t seem to work either.
New Postulation
After thinking about it, the possible way that the lockup could be having the effect we see is that it
- Doesn’t affect the rate of spread of the virus, but instead tends to make society appear to be “smaller” than it is otherwise
- That it tends to INCREASE the socialising with vulnerable people, massively increasing the death rate.
The Size of Society
So, key here, is that somehow lockup effects the apparent “size” of society (or those able to be infected( as “viewed” by the virus
Addressing the “size” of society, imagine that you have a gun and randomly fire bullets onto a target (where they lodge). If you keep firing at the centre, soon the centre is filled with a casing of bullets that protect the target, so that it can no longer be hit. So, the more concentrated your fire, the more rapidly the layer of bullets grows until the target is not being hit. So, bullets constantly fired at the same place, are stopped more rapidly than bullets fired so as to be spread out.
Now, imagine the virus is taking a path through society, being spread from one person to the next. If that path goes through people who have already been infected, then that “path” becomes blocked, and the virus dies out. And, if like the target, the majority of those paths are concentrated through one particular area, the point at which they target stops being hit, or the virus starts disappearing, is that much quicker.
It is often said, that in society we are so interconnected, that we each know someone who knows someone, who about 6 connections or so later, knows everyone in the world. So, it would appear almost impossible to stop the virus spreading to everyone.
However, it only requires one person in that chain to have already had the virus, for that chain to break down. And when a virus hits, the key people who have a huge number of social contacts, rapidly get infected, so that very quickly society breaks down into small communities, each linked to other communities by people who have already been infected. In that way, perhaps 80% of society becomes “unlinked” to the rest of society, because the links between these groups are people who have already become immune through early infection (because they are so linked they inevitably get it early).
Now, these subgroups are not necessarily geographic. They may be people who live side by side with their neighbours, but who socialise with a subgroup of their locality because they just like each other (or go to the same church, or have children at the same school).
However, we do not all belong to one subgroup. Instead, we all belong to numerous different subgroups. Family, religion, school, work. And, depending on what we are doing, these subgroup “networks” change. So, it would appear that there are so many numerous possible pathways by which the virus can spread, that it should be impossible to stop it. The problem for the virus, is that people tend to get ill and then withdraw from society. They also only meet some subgroups relatively infrequently. So, although there is a potential to spread the virus, the person who gets ill, either “goes to bed” and stops spreading it to anyone outside their household, or doesn’t meet anyone new until after they are infectious. And now, rather than spreading the virus, they are a break in the infectious chain. So, although we are all massively connected within society, the relatively inefficient spreading of the virus, ensures that rapidly some communities are cut off from others because all the bridging contacts are immune. Thus, although it would not be possible to see that they are cut off, from the point of view of the virus, there is no person-to-person contact which allows the spread of the virus into the community. Which then means they are effectively isolated from the rest of society, and as such, it is as if the size of the vulnerable number of people is much smaller – as if society has shrunk.
A conceptual Model
Imagine you have a load of same sized balls (like atoms) that neatly fit into a huge cubic contain so as to form a checker-board pattern (similar to the salt or NaCl crystal shown to the right). Now imagine a game a bit like checkers, but where the pieces move randomly to the adjacent places/atoms, but if the random move is to an place/atom which the the piece has already been, then it gets eliminated (akin to an infected person can’t infect someone who has already been infected).
(similar to the salt or NaCl crystal shown to the right). Now imagine a game a bit like checkers, but where the pieces move randomly to the adjacent places/atoms, but if the random move is to an place/atom which the the piece has already been, then it gets eliminated (akin to an infected person can’t infect someone who has already been infected).
It is quite obvious that if we start the piece in a random location, then because each position is connected to six other positions, at least one of which must have been occupied previously. Then there is higher than a one in six chance that the piece will be eliminated each time it randomly moves.
So, let’s change the rules, that everyone so often we not only move the piece to another place/atom, but we also increase the number of pieces, allowing the second to move to a new position to the original, so that initially the number of pieces moving each go tends to increase rapidly. Now, there is a very good chance that the pieces will spread in all directions so as to be able to reach anywhere that has not been previously infected.
But, anyone who has played games or puzzles, like this, also knows that although it may seem easy to reach everywhere, sometimes areas of the “board” or atoms in this case, get cut off because every position surrounding them has already been “taken”. Also, pieces can move into “dead ends” so that they can get into a space, but there is no way out. Thus, when sufficient amounts of the matrix have already been occupied (infected), there can be a large number of places/atoms (people) who have not been occupied (infected). Depending on how atoms are connected, the ease of creating these “unreachable” spaces changes. But it would be expected that a substantial fraction of space eventually become unreachable. From a traditional virology point of view, these “spaces” which cannot be reached, appear to make the size of the epidemic, and therefore “size of society” smaller than it would otherwise be.
This model uses a very simple “topology” of connections. In a real society, this “topology” is far far far more complex. Indeed, the topology of connections has a time element, so that they tend to change on a daily, weekly and even yearly cycle. However, it is true that despite being much more complex, in the same way, “spaces” can develop which cannot be reached by the virus. And it is also true, that the complexity of this topology determines the average fraction of “unreachable space” and therefore apparent size of the society from an virology point of view.
Increasing deaths without changing the rate of spreading
How is it possible that policy does not change the rate of spread, but does change who gets the virus, so that the vulnerable now get a far larger number of the infections?
This really perplexed me, because although I could explain why anti-social policies increased deaths in the vulnerable, they also ought to have REDUCED the rate of spread, so have had an effect on the gradient of the curves.
To explain, this I finally hit on a postulated social law:
That people socialise the same amount over a given time and so the chance of spreading the virus remains constant, all government tends to change is who people socialise with, not how much they socialise.
The idea here, is that if people get told “don’t socialise with your friends”, all they do, is not to reduce their socialising, but instead to find someone else they are permitted to socialise with. Thus, if someone is the first person in their community, then the “lockup” has ZERO impact on the number of people they pass the virus onto. Instead, it simply changes WHO they pass it onto. Thus the value of R0 doesn’t change, because people socialise as much, and because caring for elderly relatives was a permitted form of socialising, the impact of stopping people meeting & so socialising with their friends and work colleagues, was that they instead went and did the same amount of socialising with close family which thereby MASSIVELY increased the transmission to elderly vulnerable people.
In other words, the impact of lockup, was not to reduce the socialising that spreads the virus, instead, it merely meant that the socialising was with perhaps a smaller group of people. So, the virus spread just as rapidly after lockup as before, but because people were meeting close friends and family (i.e those who would not snitch), the “pathways” through society were a lot more “tangled” so that they more frequently crossed over each other. So that if one pathway through society had becoming infected and so immune, it became much more likely that another pathway would “tangle” up with a previously immune pathway. The result, was much fewer pathways could be infected, so many people effectively became “detached” from the infection because the only people linking them to people who were infected had themselves got immunity. In effect, lockup made it easier to create “unreachable spaces” of people and so effectively reduced the size of society, thus changing the point of the change from increase to decrease, without changing the rate of increase or decrease.
The problem is that far more of the pathways included vulnerable people … so that many more vulnerable people got infected and so the overall death rate increased.
The Second Wave
As can be seen from the top curve, the, or perhaps “an” epidemic took off. (With a peak occurring about the 23rd November).
This is yet another extremely difficult thing to explain, because how can the first epidemic have died out as if it had reached community immunity, but then a new one have started?
Again some possibilities
- That it’s fake (false positives)
- That it’s a fake (totally fake figures)
- That it’s a new variant of covid
- That it’s a different epidemic being mistaken for covid
- That society “reconfigured” so that entirely new set of pathways came about so that it is as if there were a new community of uninfected people
I suspected the first for a long time, but the rate of growth should have matched the growth in testing and it did not.
It is quite possible we are being lied to – the easiest to explain, is blatant corruption trying to keep the epidemic supposedly going until a vaccine arrives, but why then allow it to peak?
It is possible, that a new variant of covid evolved, to which many people have partial immunity. So, it is spreading, but not as well as the original variant.
I am quite convinced that the PCR test is very poor as discriminating between genetic code, so I could be easily persuaded that a completely different bug is being picked up and wrongly labelled as Covid.
The last is interesting. The idea, is that the key “bridges” in society that link groups, have changed so that the bridges are no longer being filled by people who got immunity, so that subgroups are now reconnected to the rest of society. This might be because we change our activities from summer to winter, so different people then act as bridge. It might be when students go to University, this effectively “changes all the railway points”, so it is as if there are completely new pathways through society for the virus to spread along. Or, it may be that given time, people move on. So, it’s not that there was a sudden change, just that in the time the epidemic dropped to almost nothing, enough people changed in these key “linking” positions in the chains, that sufficient groups who had been isolated, now became linked together to allow the virus to spread anew.
Going back to the analogy with the balls in a “salt matrix”, imagine if the bucket with the balls, were to be emptied out into a new bucket so that all the balls got completely jumbled up. But also imagine that there were still many “virus” pieces in the game. Now, because the pieces are mixed up, previously blocked areas have been reconfigured so that they are no longer “unreachable” and so can be “infected”. This is the analogy that might explain the second wave. We just “reconfigured” society so that people who were previously protected by an impenetrable wall of previously infected people, now had new social contacts, which did not protect them, and instead linked them to the epidemic.
