
 Around 400 people drown each year in the UK, so one might assume that there is a CONSENSUS about how people should treat people who have drowned. And that CONSENSUS is that “an abdominal thrust should be performed only after ventilation has been shown to be ineffective and then only to remove a solid foreign body.”
Around 400 people drown each year in the UK, so one might assume that there is a CONSENSUS about how people should treat people who have drowned. And that CONSENSUS is that “an abdominal thrust should be performed only after ventilation has been shown to be ineffective and then only to remove a solid foreign body.”
(Climate sceptics will immediately spot that I’m flagging this as highly suspicious by referring to the “Consensus” – because in climate this usually means scientifically baseless)
However this consensus appears to be in sharp contradiction to the evidence:
“There have been numerous reported cases which state that the Heimlich Maneuver worked when all other lifesaving measures failed. In fact a Patrick Institute study found that in a series of unconscious, non-breathing pulseless drowning victims, 87% survived when the Heimlich Maneuver was performed, whereas only 27% survived when CPR was performed without the Heimlich Maneuver. According to University of Houston Professor John Hunsucker, in a study conducted for the National Pool and Waterparks Association, that in 27 drowning incidents reported by NPWPA trained lifeguards, 24 victims responded by breathing from the Heimlich procedures alone and only three required CPR after the Heimlich was administered.”
So the evidential base (if this is a correct appraisal of that evidence) is very clear: the Heimlich manoeuvre works and the evidence appears to totally contradict the expert CONSENSUS.
So, it is very interesting to read why the “experts” appear to reject the evidence (see The Heimlich Controversy in Near-Drowning Resuscitation). These seem to fall into the following categories:
- The consensus says otherwise – reading between the lines, this is a debate sparked by discussion on the internet where the “powers that think they should dictate” long ago decided the views on the internet were wrong and should never be allowed to be heard.
- There’s too much work/loss of face involved if we change our minds: “the prospect of teaching rescue workers a different protocol than that which is taught at present for resuscitating victims of cardiopulmonary arrest from all causes other than drowning.”
- Lack of understanding trumping the evidence. It is clear the experts don’t understand why Heimlich appears to be more effective than their own preferred mechanism. But rather than accept the evidence Heimlich works, it appears they reject it in favour of mechanisms that they think they understand which has a lower success rate.
- A theoretical rejection of the perceived mechanism by which it is assumed that Heimleich works taking precedence over the practical fact it does work.
- A failure to understand that Heimlich is also a means of ventilation so the assumption the Heimlich manoeuvre is delaying ventilation “the amount of time it would take to repeat this manoeuvre until the patient is no longer expelling water (as recommended by Heimlich) and how long this would delay the initiation of artificial ventilation”
- Extreme examples where it is just possible that Heimlich might be worse being used as proof it is always worse: “possible complications of the Heimlich manoeuvre, especially if the near drowning is associated with a cervical fracture” (aka is it better to be dead with a cervical fracture or alive but paralysed because Heimlich was used the rare case where this might create a complication).
- Not Invented here – whilst there is no explicit evidence in the article, the behaviour is symptomatic of groups who reject ideas from outsiders.
The climate debate
And the reason I am posting this, is because it is so reminiscent of the climate “debate”. The fact is that like Heimlich, predictions of the climate based on the concept of “natural variation” outperform all other theoretical models in practice. However, these are overwhelming rejected by academics in favour of appalling bad models which are contradicted by the climate data but which they believe they understand.
So, experts – who publish in journals and live in ivory towers of academia – prefer theoretically “correct” models that are wrong in practice. Whereas actual life guards – who have to deal with real deaths – only care about which work best in practice.
There is something fundamentally wrong with the culture of academia or wherever these self-appointed experts come from which seems to me to be anti-common sense and as far as I can see from the evidence is literally killing people by dictating that theoretically right but practically useless methods/models must be used.
Addendum
This is turning into a fascinating case and fortunately one where I’m hopefully a dispassionate bystander.
I’ve now come across, a webpage (http://medfraud.info/Experts.html) in which all the vitriol typical of the climate debate is seen. This comment seems to sum it up:
I don’t care how many lives the Heimlich maneuver saved. That doesn’t give you a license to go overseas and inject people with poor medical care
It seems to be generally agreed that the manoeuvre known as Heimlich does save lives, but this has not prevented what appears to be a massive campaign of hate against him. Is this justified? To sum it up:
- It is disputed whether Heimlich “invented” the manoeuvre – I personally don’t care who invented it as this does not change whether it works. But for some people this appears in itself to be enough to discredit it.
- Heimlich makes lots of other claims – many seem odd. But having seen the way the establishment machine sets out to destroy those who do not comply – I would need to investigate each and every one to know what credibility there is or is not to these claims.
- There is no doubt that the Stomach compression technique saves lives. There appears to be evidence that if people were to be taught only one technique for choking and drowning, then stomach compression is a good technique in extreme cases. But if someone is chocking I would naturally slap people on the back first – and only use stomach compression if things were serious (I’d also be yelling for an ambulance).
Insert to Addendum
After finding some very negative comments I added this addendum, but then continued searching to check whether the statistics on the effectiveness of the stomach compression technique were valid and found this: http://www.aquaticsintl.com/research/dangerous-maneuvers.aspx
Now that I’m convinced there is good evidence for stomach compression, I’m putting this before the “witch hunt of heimlich” which is relegated to the end.
Yes there is good evidence supporting the use of the stomach compression technique and yes it does look like a witch hunt against practitioners who know their technique works against idiot academics who think everyone should listen to them because “they know best”.
And it does make sense. Drowning is fundamentally a loss of oxygen to the brain which in turn shuts down the respiratory system, both lungs and heart. So the sooner fresh air and heart compression is used, the more likelihood of survival.
A long time ago I was taught life-saving. I was taught to give mouth to mouth resuscitation in the water and I’ve always known it was a totally useless thing because if I’ve just swum out to some victim as fast as I am able I simply would not have the breath be able to do anything useful.
I know that the fastest I can swin 25m is around 30seconds. But 100m takes around 160seconds. So, just for me on my own to swim out to a victim some 50m out from shore and get back would take around 3minutes. So realistically it would be several minutes between reaching a drowned person and getting them to shore. But these are crucial minutes during which I knew I was unable to give the life-giving air they needed which would likely be the difference between life and death. So now if the worst were ever to happen, I have something I could do which would mean I was bringing back someone who had some fresh air in their lungs and might be worth me risking my own life to save them.
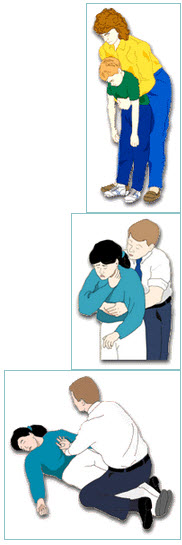
All I do is get behind them, lift their face out the water and give them 5 quick compressions – exactly where is probably dictated more by what is practically possible rather than what is theoretically best.
And time really is the crucial element and not theoretical claptrap about what is “best”. This is what an actual drowning incident is like:-
MagiDidymusJames 123 points 1 year ago
When I was twelve I drowned in the gulf of Mexico. I was out pretty far from my family and the current picked up into a rip. I had always been a very strong swimmer and I knew what to do: swim parallel. On this occasion I wore myself out and started to sink beneath the water. I remember struggling to breathe. Then, I took a big breath of water and everything stopped. The only way I can describe it is by saying it was being at Zero. I wasn’t scared or excited. I was just Zero. I was looking through the water and I blacked out. During that time, my mother was swimming out to me (she’d been a surfer all her life) and pulled me to shore and gave me CPR until I coughed up water.
It takes time to get to someone and time to bring them back. This person drowned in view of their parents who were trained in life-saving and making their way out to them. That time – without any fresh air in the lungs – is the difference between living and dying. How can academics sit in their ivory towers telling those with experience what they should or shouldn’t do when I’ve no doubt many of these academics have no practical rescue experience.
So, I was pleased to find this:
NASCO’s position
In 2010 Hunsucker published a report in the International Journal of Aquatic Research and Education, which explains NASCO’s position. He followed that report last year with a public statement. But medical experts and reports in the popular media have continued to question NASCO’s practice.
NASCO was founded in 1974, and the current protocol has been in place since the mid- to late 1990s, according to the 2010 IJARE report that Hunsucker co-authored with Scott Davison, vice president of development at NASCO. Hunsucker holds Ph.D.s in mathematics and engineering.
NASCO’s protocol has six major parts: scanning, victim identification, moving to the victim, in-water intervention (IWI)/removing the victim from the water, out-of water intervention (including CPR), and management, as described in the paper. The Heimlich maneuver comes in as an in-water intervention technique, defined in the paper as “applying a resuscitation procedure in the water, immediately after contacting a drowning victim.” The company advocates the use of five (and only five) abdominal thrusts in cases of short-duration submersion (one minute or less), while the victim is still in the water. That procedure should be followed immediately by extricating the victim from the water and performing CPR according to American Heart Association protocols.
“These thrusts delay extrication between four to six seconds,” NASCO stated in the open letter on the subject, dated Oct. 30, 2011. “The intent of these thrusts is to begin to initiate respiration.”
To define the effectiveness of NASCO’s use of the technique, Hunsucker and Davison’s IJARE report analyzed data from waterpark client rescue reports dated between 1999 and 2009. These included 56,000 rescues and 32 respiratory failures resulting in four deaths.
Those findings show that the NASCO protocols including the use of abdominal thrusts resulted in restored spontaneous respiration in approximately 87 percent (28) of respiratory failure victims. Spontaneous respiration was restored using just IWI in 14 (nearly 44 percent) of the 32 respiratory failure cases, and abdominal thrusts done out of the water restored spontaneous respiration on two other cases.
The ongoing dispute
NASCO has received a significant amount of criticism for its position recently.
In 2009, three fatal drownings at NASCO facilities raised the issue of NASCO’s use of the Heimlich in the popular media. Last year, the Northern Virginia Park Authority eliminated the use of the Heimlich in its lifeguard rescue protocols after a story in the Washington Post made the general public aware that the technique had been discredited by the medical community as an acceptable protocol for drowning resuscitation.
“All of us in the emergency medical field — whether first responder, EMT, paramedic, whatever — are not the ones who set the protocols. The protocols are set by medical experts, and it’s our job to follow those protocols. Period,” says B. Chris Brewster, president of USLA. “If, for example, a paramedic is involved in some sort of emergency intervention and takes actions that are inconsistent with the protocols, it’s a major violation of professional ethics.”
The question of ethics was raised by respected experts, including Wernicki, Peter Chambers, Roy Fielding, Terri Lees, David Markenson, Francesco Pia and Linda Quan, in rebuttal to NASCO’s IJARE article. The rebuttal, published in IJARE in 2011 stated that “the study failed to adhere to all three recognized principles of human subject research — autonomy, beneficence, and justice. …”
“The study was ill-conceived and poorly carried out,” Wernicki summarizes. “The purported outcomes do not support the conclusions stated. The review of the literature is incorrect and misleading. It unethically subjected thousands of children and adults to a universally condemned procedure. It had no oversight or approval by any scientific board. It was performed on unsuspecting subjects who never gave informed consent. The study authors had significant conflicts of interest and potentials for bias.”
For his part, Hunsucker continues to maintain the position that abdominal thrusts work as an in-water intervention technique that is a small part of the overall NASCO response protocol. He points out that NASCO’s drowning rate of 0.00635 per 100,000 compares favorably with the CDC estimate for all pool drownings of 0.6 per 100,000.
This appears to be an eminently sensible approach based on the evidence and I think they are quite right to ignore the academic theoreticians. But apparently like Mann some of these theoreticians have the ear of the press. But this clip seems to sum up the evidence well without overly taking sides:-
(back to original addendum)
This article is supposedly written by Heimlich’s son, however if it is by his son, whilst it may contain real evidence, it seems far too sensationalist and looks like his son inherited some of his father’s need to get attention:-
Medical experts speak out against my father’s history of misconduct
Robert S. Baratz MD PhD DDS, National Council Against Health Fraud:
(Henry Heimlich’s career) is the biggest case of scientific fraud I’ve ever seen. The longest, the biggest and the most far-reaching, without a doubt…His ideas are insane. Some of his ideas are delusional. He has been experimenting on human beings for most of his career, and he’s no different than the Nazi experimenters. There isn’t one iota of scientific basis for this except that Heimlich said so. (source)
Joseph P. Ornato MD, Medical College of Virginia:
Dr. Heimlich continues to distort, misquote, fabricate, and mislead his peers and the public regarding the scientific “evidence” supporting the safety and efficacy of his (drowning) theory. Dr. Heimlich’s “evidence” consists of unsubstantiated, poorly documented anecdotes. He cites letters to the editor (published in the Journal of the American Medical Association) as though they represented rigorous scientific study. (August 1992 letter to the American Red Cross as quoted in the Cincinnati Enquirer, May 10, 1993)
He almost got me fired. The things he was saying about me were really slanderous. (source)Peter Lurie MD, Deputy Director, Public Citizen’s Health Research Group
I don’t care if you’re Henry Heimlich. I don’t care how many lives the Heimlich maneuver saved. That doesn’t give you a license to go overseas and inject people with poor medical care with dangerous microorganisms. (source)
James P. Orlowski MD, Tampa University Community Hospital:
He called me a liar and said I was totally unscientific and didn’t understand how important his maneuver was…(Heimlich is) an obstructionist…His approach has been to prevent the studies from ever being done, so nobody can get an answer to whether he’s right or wrong. (source)
Linda Quan MD, Seattle Childrens Hospital:
His mischaracterization (of my study), in print, was grossly misleading and defines his character. (source)
Charles W. Guildner MD (ret), former consultant, American Heart Association:
It’s so repugnant to me the way Dr. Heimlich has bullied..He’s a bully and he has bullied people into submission. (source)
Roger D. White MD, Mayo Clinic, American Heart Association consultant:
Heimlich overpowered science all along the way with his slick tactics and intimidation, and everyone, including us at the AHA caved in. (source)
Jerome H. Modell MD, University of Florida, Gainesville:
Inclusion of the Heimlich maneuver in the 1985 (American Heart Association drowning) protocols was a concession to Heimlich. (source)

One of my favourite arguments against consensus is the point that at one point it was believed that pumping cigarette smoke up a drowning victim’s bottom might revive them. Kits for administering this were placed along the Thames. Ramming the cigarette lobby down our throats at every opportunity, draws the threads together.